You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
4/20 Cobb AMPS(+15) 350 +3.75 268 +7 159 PMPS 209
- Thread starter Suzanne & Cobb(GA)
- Start date
- Status
- Not open for further replies.
Kim & Twice
Member Since 2013
Re: 4/20 Cobb AMPS(+15) 350
Good morning Suzanne") Happy Easter!!
Happy Easter!!

Sending good Vetty vines for tomorrow, and dental vines too
Hope you're having a great visit with your folks!
Good morning Suzanne
Happy Easter!!Hmmm....Do YOU see the common denominator here??? :lol: :lol:Matty is actually adjusting very well. He's sleeping better here than he does at home. Wait a second...Matty is sleeping better, Cobb's numbers are better...this place must be more calming than I think...strange, it wasn't like this when I was a teenager... :lol:
Sending good Vetty vines for tomorrow, and dental vines too
Hope you're having a great visit with your folks!
Re: 4/20 Cobb AMPS(+15) 350 +3.75 268
Not bad at all. Great job using the R.

Not bad at all. Great job using the R.
Re: 4/20 Cobb AMPS(+15) 350 +3.75 268 +7 159
Great to see those blues back again!
I hope you enjoyed the early service and you all are having a great Easter.
Tons of good vetty vines coming your way for tomorrow.

Great to see those blues back again!
I hope you enjoyed the early service and you all are having a great Easter.
Tons of good vetty vines coming your way for tomorrow.
rhiannon and shadow (GA)
Member Since 2012
Re: 4/20 Cobb AMPS(+15) 350 +3.75 268 +7 159

Suzanne & Cobb(GA)
Member Since 2013
Wow! Cobb cleared that bounce quickly! He's been pretty good this weekend. Growling and hissing but, based on his BG, he isn't too stressed. Maybe I was overly concerned...
Vet tomorrow morning. I won't post until after the appointment since his appt coincides with Tomorrow's shot time. Hoping it all goes well and we can be in and out, and get the dental over and done with!
Vet tomorrow morning. I won't post until after the appointment since his appt coincides with Tomorrow's shot time. Hoping it all goes well and we can be in and out, and get the dental over and done with!
Tricia Cinco(GA) & Harvey
Member Since 2011
Nice slide for Cobb today. I hope you are having a wonderful celebration with your family.
Sending good vetty vines and prayers for tomorrow.
Sending good vetty vines and prayers for tomorrow.
Chris & China (GA)
Member Since 2013
Sending lots of good vetty vines for tomorrow! (While I can!...the board is being awfully glitchy tonight!)
I'm glad you're able to get him into a vet that you know and trust. That will make it easier on both of you!
Open wide Cobb!!
I'm glad you're able to get him into a vet that you know and trust. That will make it easier on both of you!
Open wide Cobb!!
Sandy and Black Kitty
Member Since 2009
Hi there 
Sending vines for a good dental Cobbs way!
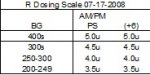
Regarding R scale questions (in your 04/17 condo):
Below is an example of one of BKs R scales, L dose was 8u at that time.
( Note to all- this was about 2 weeks out from his second hospitalization for DKA)
Using a chart really helped keep it all straight - BG range/timing/dose - not only for me but for DBF too since he was back up shooter. I kept a copy of the R scale in play taped at eye level in the area where I prepared BKs syringes. The charts also provided a chronological history of R use , which helped in making subsequent scales as the picture changed.
• Injected insulin first gets bound to the antibodies. Any insulin that does not get bound goes toward metabolizing sugars. How much goes to antibodies and how much goes to metabolizing sugars is anybody’s guess and a moving target
• IAA can retard the initial rise of available insulin after an injection.
• IAA can lead to an increase in the half-life of free (unbound) insulin in circulation because some bound insulin gets released into circulation. The increase in half-life can lead to prolongation of action.
• The release of insulin from the antibodies can happen at inopportune times
all those variables make consistency and/or predictability tough. With experience in time you will develop a sense of the ebb and flow of it all with Cobb
The scale serves as a guide. There will be times when your gut tells you to stray one way or the other from the scale.
Sending vines for a good dental Cobbs way!
Regarding R scale questions (in your 04/17 condo):
That’s really the only way it can be done - experimentation and close observation. It’s extremely situational and nuanced and will never be perfect or static.Suzanne & Cobb said:I am using more R. I'm still trying to figure out a sliding scale...kind of in the experimental phase of that right now.
You are on the right track. I recommend well-defined BG/dose ranges for safety and to assist with the inevitable tweaking.Suzanne & Cobb said:What I'm trying to do is...if he's over 300, at least 1-1.5units. He was particularly high this morning, so I gave 2 units. Then around +6, I've been following up with half of the original dose, if he is still above 250...but I may lower than to 200 and if he's between 200-250, give .5unit.
Below is an example of one of BKs R scales, L dose was 8u at that time.
( Note to all- this was about 2 weeks out from his second hospitalization for DKA)
Using a chart really helped keep it all straight - BG range/timing/dose - not only for me but for DBF too since he was back up shooter. I kept a copy of the R scale in play taped at eye level in the area where I prepared BKs syringes. The charts also provided a chronological history of R use , which helped in making subsequent scales as the picture changed.
Some things about IAA to keep in mind:Suzanne & Cobb said:I'm a little confused on how to do a sliding scale though...because I don't see that he responds to R consistently or predicably. Maybe I'm missing that.
• Injected insulin first gets bound to the antibodies. Any insulin that does not get bound goes toward metabolizing sugars. How much goes to antibodies and how much goes to metabolizing sugars is anybody’s guess and a moving target
• IAA can retard the initial rise of available insulin after an injection.
• IAA can lead to an increase in the half-life of free (unbound) insulin in circulation because some bound insulin gets released into circulation. The increase in half-life can lead to prolongation of action.
• The release of insulin from the antibodies can happen at inopportune times
all those variables make consistency and/or predictability tough. With experience in time you will develop a sense of the ebb and flow of it all with Cobb
The scale serves as a guide. There will be times when your gut tells you to stray one way or the other from the scale.
I wish I could give some slick formula but the truth of the matter is we were flying by the seat of our pants . One thing I was mindful of was the higher the L dose the larger the depot. When the IAA broke BK was at 13.5u L. He went flying down the dosing scale. Keeping ahead of the depot action was difficult - like trying to rein in wild horses. Many sleep deprived nights of endless pokes.Suzanne & Cobb said:I know at one point you were using like 11uL and 7uR, or some kind of combination like that...Bhow did you decide to up the R versus the L?
What it says is that particular combination of R and L doses was correct at that time. The L likely would not have accomplished the same results without the influence of the R.Suzanne & Cobb said:I'd prefer to keep his L dose where it is, or lower and use more R if that's a possibility. Sometimes once the R kicks in, the L does a fine job of keeping him low or bringing him lower so it says to me that the L dose is correct at that time. Or am I misunderstanding that?
Yes, you could try using R at PS only , increasing in small increments and see how Cobb reacts. That’s a good starting place. If it does not give the desired result, then you think about different approach.Suzanne & Cobb said:Or should I be using the L to treat the nadir and the R to treat the higher preshots? So if his AMPS is in the 300s, give more R and then see how the L works once the R wears off? Does that make sense?
Attachments
Tina & Rocky
Member Since 2013
Sending you and Cobb some white diamond healing light for Cobb's dental surgery tomorrow. o")
- Status
- Not open for further replies.