
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Journey continues for Ottie - CKD and Diabetes
- OP Kili
- Start date
- Status
- Not open for further replies.
.:. in.active .:.
Member Since 2023
Can you post the pictures of the syringes in the part 3 thread please?
I did it with a U100 too, but the principle is the same. In fact, my U40s had a skinnier plunger, and the syringe itself (its wall) wasn't as thick, so made it easier to fine tune the dose.
0.5 - plunger top is aligned with the 1/2 mark line
0.25 - plunger top is half way between bottom of line zero and the 1/2 mark line (there is a hairline of greenery between the zero line and the plunger top)
0.1 - the plunger top touches the bottom of the zero line - side view to show that there is some green liquid in the syringe
empty - there is nothing in the syringe, plunger touches the top of the zero line (that empty hairline you see above the plunger is just the perforation - there is no space/air there for a "drop" suction previously discussed)
I'm not really sure whether it helps make things clearer. If you guys disagree with the explanation or execution, let me know and I delete the images.
(Edit: wow, all zoomed in it looks like a skinny 0.25, but I don't have my contacts in and I'm blind without them
 )
)Attachments



Kili
Member Since 2023
I also said:
“Just for me trying to figure out how he ended up at 45 today at +4, can you please tell me what and when he ate leading up to the lime green 45. He should have been eating snacks of low carb wet food every hour or so between shot time and +4. When he hit the lime green 45, what did you feed him?”
On this topic... Ottie was grazing since 3am all the way to 8am when he had his 0.25U shot. So he ate quite a bit (for his standard) prior to the shot. Post shot after 8am, he had some food, but the volume he was eating dropped... and it was hard to get him to eat anything. I feel that this is the main problem... Esp during the morning/lunch... He doesn't want to eat as much. Less problem at night, where he has more of an appetite.
03:30 Food
04:05 More Food
05:10 Food
06:00 Food
06:20 Food
07:42 11
07:48 Food
08:00 Food
09:40 Food (did not finish food from 0800, added a little more on top)
10:00 Food (added on top of last batch... still did not finish)
09:50 7.3
At this point, I thought he was just full, and didn't want to eat.
12:00 2.5 (pure panic erupted... I tried desperately for him to eat... He refused)
Then I bought out the carb rich food that he loved. Luckily... he hoovered that down.
Ottie appeared normal on the surface... just refused to eat, until something more tasty came out.
You can see that my sheer panic boosted his BG from 2.5 to 9.9. I obviously gave him more than he needed... but at the moment, I am not sure how much I need to give to bring him out of the danger zone.
Today was really emotionally draining... I know it sounds stupid, but I'm quite traumatised by the experience of hypo. Hypo is something that I have been really scared of, since this diabetes journey started.
Last edited:
.:. in.active .:.
Member Since 2023
I said it previously, that I think we haven't seen his true potential on 0.25 IU yet, that is, if ProZinc is known to have an overlap/carryon effect, like depot insulins, since it was always administered after a 0.5 IU.
We only see the big +4 drop in his AM cycle on 0.25 IU, but based on the limited data trend, he may have gone that low on the previous 0.25 IU PM cycle, we just don't know about it.
Since you didn't shoot this PM gone, we could see what is he really like on 0.25 IU tomorrow AM, because if there is/was a depot/storage in his system, it'd have been likely drained by the morning.
On this one occasion, given the nature of the situation, although we adjust dose based on nadirs, I personally would make it dependant on his AMPS.
If he was my cat I would shoot him with 0.25 IU if his AM BG was equal or above 12.0 mmol/L, and shoot him with 0.1 IU anywhere below that.
However, if you can not monitor him throughout the AM cycle, and/or you're worried about him dropping again, then your best bet is playing it safe with 0.1 IU. But doing so, whether it's going to be his perfect dose, or a dose not doing much for him, you will need to hold that 0.1 IU for 7 days.
I'm bracing myself for getting my butt chewed for this, but...
Since you said to me that you only drew one drop of blood at testing (the first drop tends to read slightly lower -on AT2 and FSF Lite anyway, as per my experience-) and you said he was walking around, being his happy self even during that 2.5 drop at +4, I would take the gamble of 0.25 IU on my cat above a 12 mmol/L pre-shot. It can always be dropped to 0.1 IU for the PM cycle if it is indeed proven to be too much, but it would take a week of 0.1 IU to adjust the dose higher.
What is important now, is that whatever you decide to do, stick to please. These randomly skipping shots due to inconvenience malarkey definitely needs to stop! (Unless for obvious reasons, per protocol.)
I know it's a very wishy-washy reply, if anything, I'm just thinking out loud, brainstorming at 2am. Ultimately, he is your cat, you know him best, so the decision will always be yours.
I let the others lead you, because they're more experienced with this specific insulin, and I'm clearly just rambling now.
We only see the big +4 drop in his AM cycle on 0.25 IU, but based on the limited data trend, he may have gone that low on the previous 0.25 IU PM cycle, we just don't know about it.
Since you didn't shoot this PM gone, we could see what is he really like on 0.25 IU tomorrow AM, because if there is/was a depot/storage in his system, it'd have been likely drained by the morning.
On this one occasion, given the nature of the situation, although we adjust dose based on nadirs, I personally would make it dependant on his AMPS.
If he was my cat I would shoot him with 0.25 IU if his AM BG was equal or above 12.0 mmol/L, and shoot him with 0.1 IU anywhere below that.
However, if you can not monitor him throughout the AM cycle, and/or you're worried about him dropping again, then your best bet is playing it safe with 0.1 IU. But doing so, whether it's going to be his perfect dose, or a dose not doing much for him, you will need to hold that 0.1 IU for 7 days.
I'm bracing myself for getting my butt chewed for this, but...
Since you said to me that you only drew one drop of blood at testing (the first drop tends to read slightly lower -on AT2 and FSF Lite anyway, as per my experience-) and you said he was walking around, being his happy self even during that 2.5 drop at +4, I would take the gamble of 0.25 IU on my cat above a 12 mmol/L pre-shot. It can always be dropped to 0.1 IU for the PM cycle if it is indeed proven to be too much, but it would take a week of 0.1 IU to adjust the dose higher.
What is important now, is that whatever you decide to do, stick to please. These randomly skipping shots due to inconvenience malarkey definitely needs to stop! (Unless for obvious reasons, per protocol.)
I know it's a very wishy-washy reply, if anything, I'm just thinking out loud, brainstorming at 2am. Ultimately, he is your cat, you know him best, so the decision will always be yours.
I let the others lead you, because they're more experienced with this specific insulin, and I'm clearly just rambling now.
Last edited:
.:. in.active .:.
Member Since 2023
I have my hands in the air again. Generally speaking it isn't advocated here to use FSL strips with an AT2 meter and the more experienced members already suggested 0.1 IU to you.
Elizabeth and Bertie
Member Since 2010
Kili, just answering question from your previous thread..
- A preshot test is simply the test done before giving the insulin shot. The main reason we do preshot tests is to ensure the cat's blood glucose is high enough for insulin. Sometimes they can surprise us with a lower than expected number.What's a preshot test?
Go by the AT test results in the AT meter. The AT test strips are batch tested and coded to give more accurate results with cat/dog blood.The AT2 strip shows 10.9 whilst the FSL strip shows 13.8. Which is actually accurate? Its the same drop of blood.
Kili
Member Since 2023
Like it was discussed here previously, Ottie will be microdosing at 0.1U for the next 7 days unless he has hypo episode again.
So far his history has proven that he is very sensitive to the insulin. I never expected Ottie to go hypo with 0.25U.
Out of curiosity, has anyone had experience discussing microdosing with a vet?
So far his history has proven that he is very sensitive to the insulin. I never expected Ottie to go hypo with 0.25U.
Out of curiosity, has anyone had experience discussing microdosing with a vet?
Elizabeth and Bertie
Member Since 2010
The fact that there were no symptoms at that point does not mean there was not a risk. 'Absence of symptoms does not necessarily mean absence of hypo'. Some cats don't show any symptoms at all until the hypo is advanced or severe. But things can change quickly in hypo situations. A couple of examples...Since you said to me that you only drew one drop of blood at testing...and you said he was walking around, being his happy self even during that 2.5 drop at +4, I would take the gamble of 0.25 IU on my cat above a 12 mmol/L pre-shot.
I did a random spot check test on Bertie. His BG was 2.6 on a human meter. But it was dropping fast... He looked completely normal at that point.
In the seconds it took me to run downstairs, grab glucose, and run back up again, everything had changed. He was showing a number of hypo symptoms. He was staggering around and falling over. His pupils were completely dilated. He appeared to be hallucinating. And he'd become very aggressive which made it really hard to get glucose into him.
Another UK lady was watching TV one evening with her cat sitting next to her on the couch. Cat appeared to be completely normal.
Then the cat just fell off the edge of the couch and started having seizures. This cat showed no symptoms whatsoever until the hypo was severe...
Fortunately the lady knew what to do, and her quick actions may well have saved her cat's life.
For this reason we have to take low numbers very seriously, even if there are no hypo symptoms.
Elizabeth and Bertie
Member Since 2010
I've talked to my vet about it. She's a cat-only vet treating quite a few diabetic kitties, and she has one herself... But she has never done microdosing. And she was absolutely amazed that tiny doses worked in my cat. (BTW, she's happy for me to dose as I think necessary).Out of curiosity, has anyone had experience discussing microdosing with a vet?
Kathryn Elizabeth
Member Since 2023
If you are in that kind of situation and need to get sugar into the cat fast and they are not even in a state to eat, then what do you do?The fact that there were no symptoms at that point does not mean there was not a risk. 'Absence of symptoms does not necessarily mean absence of hypo'. Some cats don't show any symptoms at all until the hypo is advanced or severe. But things can change quickly in hypo situations. A couple of examples...
I did a random spot check test on Bertie. His BG was 2.6 on a human meter. But it was dropping fast... He looked completely normal at that point.
In the seconds it took me to run downstairs, grab glucose, and run back up again, everything had changed. He was showing a number of hypo symptoms. He was staggering around and falling over. His pupils were completely dilated. He appeared to be hallucinating. And he'd become very aggressive which made it really hard to get glucose into him.
Another UK lady was watching TV one evening with her cat sitting next to her on the couch. Cat appeared to be completely normal.
Then the cat just fell off the edge of the couch and started having seizures. This cat showed no symptoms whatsoever until the hypo was severe...
Fortunately the lady knew what to do, and her quick actions may well have saved her cat's life.
For this reason we have to take low numbers very seriously, even if there are no hypo symptoms.
.:. in.active .:.
Member Since 2023
"Out of curiosity, has anyone had experience discussing microdosing with a vet?"
I've talked to my vet about it. She's a cat-only vet treating quite a few diabetic kitties, and she has one herself... But she has never done microdosing. And she was absolutely amazed that tiny doses worked in my cat. (BTW, she's happy for me to dose as I think necessary).
I have totally missed Kili's question on this one (and now I can't seem to find it to quote):
My vet is familiar with the exact protocol I follow (TR on Lantus) and she advocates for microdosing, in fact she was the one suggesting to even try a 0.05 IU adjustment, given my cat's reaction.
PLEASE NOTE: I am using the calliper method for this, so I'm able to execute this. I see it being extremely hard to do so without one.
.:. in.active .:.
Member Since 2023
Is this all you can do during hypo? I'm specifically mentioning the part where they are squeezing syrup into the cat's mouth using a syringe to give him sugar quickly.
You can rub syrup on their gums with your finger, too.
They don't have to digest the glucose, as sugar is one of the few substances that can be absorbed by the mucus membranes (under tongue, buccal cavity, gums), I believe. Thus why simple sugars (e.g. Karo syrup) is preferred over, let's say, honey, which their system would need harder to work to break down.
You rub their gums with syrup every 10 minutes, until their BG is high enough for comfort. And even then, you ought to monitor them closely, in case they drop again. (I've experienced that happen unfortunately.)
Human study:
First aid glucose administration routes for symptomatic hypoglycaemia
Last edited:
Kathryn Elizabeth
Member Since 2023
i am a newbie here and it's taken a bit to get my head around but i think these pics are incredible!I did it with a U100 too, but the principle is the same. In fact, my U40s had a skinnier plunger, and the syringe itself (its wall) wasn't as thick, so made it easier to fine tune the dose.
0.5 - plunger top is aligned with the 1/2 mark line
0.25 - plunger top is half way between bottom of line zero and the 1/2 mark line (there is a hairline of greenery between the zero line and the plunger top)
0.1 - the plunger top touches the bottom of the zero line - side view to show that there is some green liquid in the syringe
empty - there is nothing in the syringe, plunger touches the top of the zero line (that empty hairline you see above the plunger is just the perforation - there is no space/air there for a "drop" suction previously discussed)
I'm not really sure whether it helps make things clearer. If you guys disagree with the explanation or execution, let me know and I delete the images.
(Edit: wow, all zoomed in it looks like a skinny 0.25, but I don't have my contacts in and I'm blind without them
View attachment 67279 View attachment 67280 View attachment 67281
Elizabeth and Bertie
Member Since 2010
For more info on hypo see FDMB's hypo file here:
https://www.felinediabetes.com/FDMB/threads/how-to-treat-hypos-they-can-kill-print-this-out.15887/
Note: Most of the numbers here are human glucose meter numbers. So if using a pet meter such as Alphatrak those numbers would probably be a tad higher (pet meters 'typically' read a bit higher than human meters and vice versa).
https://www.felinediabetes.com/FDMB/threads/how-to-treat-hypos-they-can-kill-print-this-out.15887/
Note: Most of the numbers here are human glucose meter numbers. So if using a pet meter such as Alphatrak those numbers would probably be a tad higher (pet meters 'typically' read a bit higher than human meters and vice versa).
Last edited:
Kili
Member Since 2023
On the topic of microdosing... It's such a small drop of insulin... that at times you even wonder whether there was anything that went in to the kitty.
To those who are more experienced with microdosing... Have you gone through times, where you were sure you measured the amount, but then when you test +3hrs, the BG number went up? Which makes you wonder whether you injected that micro amount?
Coz it's such a small amount, can't help but always wonder whether I injected or not... Althouigh I spent nearly 30mins trying to load the syringe with a micro amount.
To those who are more experienced with microdosing... Have you gone through times, where you were sure you measured the amount, but then when you test +3hrs, the BG number went up? Which makes you wonder whether you injected that micro amount?
Coz it's such a small amount, can't help but always wonder whether I injected or not... Althouigh I spent nearly 30mins trying to load the syringe with a micro amount.
.:. in.active .:.
Member Since 2023
Whether you injected it or not, you never double-shoot. I'm sure you're aware of this though.
Comparing the data with your first ever (NS) PM log, the numbers look almost identical, so yes, it may have been a fur shot. But it's OK. It happens to all of us.
Mind you, BG fluctuates, and let's say if Ottie hasn't eaten much pre-shot and devoured a substantial amount of food right before you tested that +3, that can influence the numbers.
Also, remember, it's just a spot check. We are looking at trends.
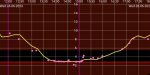
I do a lot of data analysis in my field. We are always looking at trends/patterns. I'll try to explain it with our own example, from when my cat still had the CGM on.
The bright pink/purple line is the average glucose at a given time.
The faded white/pink line is the actual glucose as and when it fluctuates in real time. This is the live stream I see on my phone, when my cat decides not to peel the sensor off him, and is close enough to me for bluetooth connection.
1. The average glucose for around 2pm is 4.3 mmol/L but
2. The actual glucose at 13:47 was 6.1 mmol/L and
3. at 13:58 was 3.1 mmol/L (I didn't take a screenshot, but you can clearly see, that it has gone back up to about 5.0 mmol/L by ~14:05)
Therefore it all depends on when you do the ear prick. If you do it at 13:47 you see a different number than if you did it 10mins later. Glucose changes by the minute, as you can see.

And when you do not have the luxury to live-stream your cat, you spot check. (Like shown below.)
And quite literally, you connect the dots, to see the pattern/trend. That's why I told you before, it's important to "fill the gaps".

I guess what I'm trying to say is, that maybe his +3 was higher than his PMPS, but we do not have enough spot checks yet, to connect the dots and see a clear trend, regardless of whether or not it was a fur shot.
I'm also wet- and smell- check my cat's fur after each shot, just to be safe. Not sure whether the latter would work with ProZinc though. Lantus has an incredibly strong smell, so you can smell it from miles away. I used to buzz the shooting site too, when we first begun on this journey. Less hair, more chance to get the shot right. I'm also using 13mm needles, as I'm not comfortable with the shorter 6 or 8mm ones, because my boy has long ish fur.
Comparing the data with your first ever (NS) PM log, the numbers look almost identical, so yes, it may have been a fur shot. But it's OK. It happens to all of us.
Mind you, BG fluctuates, and let's say if Ottie hasn't eaten much pre-shot and devoured a substantial amount of food right before you tested that +3, that can influence the numbers.
Also, remember, it's just a spot check. We are looking at trends.
I do a lot of data analysis in my field. We are always looking at trends/patterns. I'll try to explain it with our own example, from when my cat still had the CGM on.
The bright pink/purple line is the average glucose at a given time.
The faded white/pink line is the actual glucose as and when it fluctuates in real time. This is the live stream I see on my phone, when my cat decides not to peel the sensor off him, and is close enough to me for bluetooth connection.
1. The average glucose for around 2pm is 4.3 mmol/L but
2. The actual glucose at 13:47 was 6.1 mmol/L and
3. at 13:58 was 3.1 mmol/L (I didn't take a screenshot, but you can clearly see, that it has gone back up to about 5.0 mmol/L by ~14:05)
Therefore it all depends on when you do the ear prick. If you do it at 13:47 you see a different number than if you did it 10mins later. Glucose changes by the minute, as you can see.
And when you do not have the luxury to live-stream your cat, you spot check. (Like shown below.)
And quite literally, you connect the dots, to see the pattern/trend. That's why I told you before, it's important to "fill the gaps".
I guess what I'm trying to say is, that maybe his +3 was higher than his PMPS, but we do not have enough spot checks yet, to connect the dots and see a clear trend, regardless of whether or not it was a fur shot.
I'm also wet- and smell- check my cat's fur after each shot, just to be safe. Not sure whether the latter would work with ProZinc though. Lantus has an incredibly strong smell, so you can smell it from miles away. I used to buzz the shooting site too, when we first begun on this journey. Less hair, more chance to get the shot right. I'm also using 13mm needles, as I'm not comfortable with the shorter 6 or 8mm ones, because my boy has long ish fur.
Attachments

Suzanne & Darcy
Member Since 2020
Shelley answered this over on the ProZinc forum. Just in case you didn't see it.On the topic of microdosing... It's such a small drop of insulin... that at times you even wonder whether there was anything that went in to the kitty.
To those who are more experienced with microdosing... Have you gone through times, where you were sure you measured the amount, but then when you test +3hrs, the BG number went up? Which makes you wonder whether you injected that micro amount?
Coz it's such a small amount, can't help but always wonder whether I injected or not... Althouigh I spent nearly 30mins trying to load the syringe with a micro amount.
Kili
Member Since 2023
Sadly, it seems like Ottie hasn't remained his old self. (He was more like his old self yesterday). He seems to be back to mopy again.
The only change that I have done since yesterday was that we changed his food from Sheba Fine Flakes to Thrive. The main reason was that I am trying to find food that is low is phosphorous for his CKD. I had to change his food a few times since his diagnosis... because Ottie will eat the food for a day or so... then completely refuse. At the moment, I am not sure how long Thrive will succeed to keep him satisfied.
So far, its looking like his insulin dose needs to be increased... but I presume I remain on course at 0.1U until 7 days is complete?
I feel deflated today to watch him back to his mopy self.
I have been doing BG testing at +3 and +6 to reduce the amount of times his ears are pricked. BUT I will have to test him more (every 2hr) when I increase dosage to 0.25U.
Since yesterday, it seems like his water drinking has slightly increased too.
Is it worth trying a dose increase earlier? Or best to carry out the 7 days cycle.
The only change that I have done since yesterday was that we changed his food from Sheba Fine Flakes to Thrive. The main reason was that I am trying to find food that is low is phosphorous for his CKD. I had to change his food a few times since his diagnosis... because Ottie will eat the food for a day or so... then completely refuse. At the moment, I am not sure how long Thrive will succeed to keep him satisfied.
So far, its looking like his insulin dose needs to be increased... but I presume I remain on course at 0.1U until 7 days is complete?
I feel deflated today to watch him back to his mopy self.
I have been doing BG testing at +3 and +6 to reduce the amount of times his ears are pricked. BUT I will have to test him more (every 2hr) when I increase dosage to 0.25U.
Since yesterday, it seems like his water drinking has slightly increased too.
Is it worth trying a dose increase earlier? Or best to carry out the 7 days cycle.
Suzanne & Darcy
Member Since 2020
I talked about his dose this morning over on your ProZinc forum thread.Sadly, it seems like Ottie hasn't remained his old self. (He was more like his old self yesterday). He seems to be back to mopy again.
The only change that I have done since yesterday was that we changed his food from Sheba Fine Flakes to Thrive. The main reason was that I am trying to find food that is low is phosphorous for his CKD. I had to change his food a few times since his diagnosis... because Ottie will eat the food for a day or so... then completely refuse. At the moment, I am not sure how long Thrive will succeed to keep him satisfied.
So far, its looking like his insulin dose needs to be increased... but I presume I remain on course at 0.1U until 7 days is complete?
I feel deflated today to watch him back to his mopy self.
I have been doing BG testing at +3 and +6 to reduce the amount of times his ears are pricked. BUT I will have to test him more (every 2hr) when I increase dosage to 0.25U.
Since yesterday, it seems like his water drinking has slightly increased too.
Is it worth trying a dose increase earlier? Or best to carry out the 7 days cycle.
Suzanne & Darcy
Member Since 2020
For lower phosphorus foods, I feed my cats Weruva BFF PLAY pate foods (chicken duck and turkey and chicken and lamb.). The duck is popular with a lot of my cats. Do you have bloodwork on Ottie that you can share? What was his BUN, Creatinine, and Phosphorus at his last bloodwork?Sadly, it seems like Ottie hasn't remained his old self. (He was more like his old self yesterday). He seems to be back to mopy again.
The only change that I have done since yesterday was that we changed his food from Sheba Fine Flakes to Thrive. The main reason was that I am trying to find food that is low is phosphorous for his CKD. I had to change his food a few times since his diagnosis... because Ottie will eat the food for a day or so... then completely refuse. At the moment, I am not sure how long Thrive will succeed to keep him satisfied.
So far, its looking like his insulin dose needs to be increased... but I presume I remain on course at 0.1U until 7 days is complete?
I feel deflated today to watch him back to his mopy self.
I have been doing BG testing at +3 and +6 to reduce the amount of times his ears are pricked. BUT I will have to test him more (every 2hr) when I increase dosage to 0.25U.
Since yesterday, it seems like his water drinking has slightly increased too.
Is it worth trying a dose increase earlier? Or best to carry out the 7 days cycle.
Suzanne & Darcy
Member Since 2020
Hold his dose for a full 14 cycles.
Suzanne & Darcy
Member Since 2020
Have you seen this food list of low phosphorus low carb foods for diabetics with CKD?
https://www.bizave.com/foodlists/CKD Diabetes Food List.pdf
I am not sure which of these foods are available to you in the UK.
https://www.bizave.com/foodlists/CKD Diabetes Food List.pdf
I am not sure which of these foods are available to you in the UK.
Kili
Member Since 2023
For lower phosphorus foods, I feed my cats Weruva BFF PLAY pate foods (chicken duck and turkey and chicken and lamb.). The duck is popular with a lot of my cats. Do you have bloodwork on Ottie that you can share? What was his BUN, Creatinine, and Phosphorus at his last bloodwork?
Weruva brand isn't something that is easy to get hold of in UK.
Last bloodtest of Ottie was held on 19th June 2023.
Sodium 151 mmol/l (140 - 157)
Potassium 4.9 mmol/l (3.4 - 5.6)
Phosphate 1.7 mmol/l (0.7 - 2.1)
Urea 20.8 mmol/l (6.1 - 12.5)
Creatinine 302 umol/l (45 - 170)
Glucose 15.2 mmol/l (3.8 - 7.6)
Kili
Member Since 2023
Have you seen this food list of low phosphorus low carb foods for diabetics with CKD?
https://www.bizave.com/foodlists/CKD Diabetes Food List.pdf
I am not sure which of these foods are available to you in the UK.
Yes... I have been through that list. The key issue is that Ottie has to like it enough to eat it. But it's one of the stresses in this journey... Ottie is picky with his food, and is not always happy with the new diet.
I tried quite a few, but like I indicated before... Ottie is keen for 1 week, then doesn't touch it.
Suzanne & Darcy
Member Since 2020
With Urea that high, it’s likely that Ottie feels nauseated and this will cause pickiness/reluctance to eat. Anti-nausea medication can really help this. If you were in the US, I would say to get some Cerenia tablets and also some Ondansetron tablets from your vet (or a script to purchase them) but my friends in the UK often aren’t able to get these meds to take home and treat at home. One friend has to take his cat to the vet for an “anti-nausea” (Cerenia) injection every time the cat feels sick. Those injections only last 24 hours! Some cats do okay on Cerenia, but Ondansetron is the most highly effective anti-nausea medication (downside is that it can be constipating and I believe you already give Ottie Lactulose for constipation.). I have had cats with CKD on both of thee medications daily.Weruva brand isn't something that is easy to get hold of in UK.
Last bloodtest of Ottie was held on 19th June 2023.
Sodium 151 mmol/l (140 - 157)
Potassium 4.9 mmol/l (3.4 - 5.6)
Phosphate 1.7 mmol/l (0.7 - 2.1)
Urea 20.8 mmol/l (6.1 - 12.5)
Creatinine 302 umol/l (45 - 170)
Glucose 15.2 mmol/l (3.8 - 7.6)
Does Ottie go up to food and sniff it and walk away— or lick the surface of the food and walk away? Any odd tooth grinding noises when he chews? These are some common signs of nausea.
Was a urinalysis done to check the specific gravity of his urine (USG) — or to check for protein in his urine?
Another really beneficial treatment that can really help a cat with CKD to feel better (because it will reduce uremic toxins and increase overall hydration and also can help constipation) is subcutaneous fluids done at home on a regular basis. This is another treatment that is pretty much standard in the US that I understand many vets in the UK do not allow their clients to do at home — and since CKD cats (when they get to the point of needing fluids) will need them daily or sometimes every other day, it’s not practical to haul the cat to the vet for these all the time. It’s sad, because fluids are one of the most important treatments to improve quality of life in a CKD cat.
I would not use appetite stimulants before first trying anti-nausea treatment, because this can create food aversion in cats (i.e., they feel hungry and yet nauseated at the same time.)
I’m happy to see that his potassium is not low. His phosphorus is on the higher end, so you are right to be trying lower phosphorus foods to spare his kidneys from having to process excess phosphorus. I’m glad you are on top of this.
Tell me, have they checked his blood pressure? A lot of vets won’t do this unless asked, but it’s very important. Many CKD cats have or will develop hypertension, which further damages the kidneys as well as other organs.
Hugs.

Suzanne & Darcy
Member Since 2020
I forgot to mention that 1.3 (4 in US) is considered optimal phosphorus level for a CKD cat.
Will he drink from a water fountain? Drinking water is very beneficial for him (although I understand that it’s distressing to see them drinking a lot of water - I tend to freak out a bit when my cats do it — assuming the worst). So make sure to add water to his food if he will allow you to and still eat it. Otherwise, fountains, dripping faucets, etc. all can get them to take in more water.
Will he drink from a water fountain? Drinking water is very beneficial for him (although I understand that it’s distressing to see them drinking a lot of water - I tend to freak out a bit when my cats do it — assuming the worst). So make sure to add water to his food if he will allow you to and still eat it. Otherwise, fountains, dripping faucets, etc. all can get them to take in more water.
Kili
Member Since 2023
With Urea that high, it’s likely that Ottie feels nauseated and this will cause pickiness/reluctance to eat. Anti-nausea medication can really help this. If you were in the US, I would say to get some Cerenia tablets and also some Ondansetron tablets from your vet (or a script to purchase them) but my friends in the UK often aren’t able to get these meds to take home and treat at home. One friend has to take his cat to the vet for an “anti-nausea” (Cerenia) injection every time the cat feels sick. Those injections only last 24 hours! Some cats do okay on Cerenia, but Ondansetron is the most highly effective anti-nausea medication (downside is that it can be constipating and I believe you already give Ottie Lactulose for constipation.). I have had cats with CKD on both of thee medications daily.
Does Ottie go up to food and sniff it and walk away— or lick the surface of the food and walk away? Any odd tooth grinding noises when he chews? These are some common signs of nausea.
Tell me, have they checked his blood pressure? A lot of vets won’t do this unless asked, but it’s very important. Many CKD cats have or will develop hypertension, which further damages the kidneys as well as other organs.
Hugs.
Ottie does sniff the food but not eat. Does not necessarily walk away though. Have not heard any odd tooth grinding noises when he chews though. However, when I put something in front of him that he used to like... He springs back to life.
So Ottie feeling lethargic is more likely to do with CKD rather than diabetes?
We have indeed checked his blood pressure and it's fine. It was 122, so was perfectly normal.
Last edited:
Kili
Member Since 2023
I forgot to mention that 1.3 (4 in US) is considered optimal phosphorus level for a CKD cat.
Will he drink from a water fountain? Drinking water is very beneficial for him (although I understand that it’s distressing to see them drinking a lot of water - I tend to freak out a bit when my cats do it — assuming the worst). So make sure to add water to his food if he will allow you to and still eat it. Otherwise, fountains, dripping faucets, etc. all can get them to take in more water.
For his CKD, we give him phosphorous binder with his food twice a day. So far we are using the Ipakitine as suggested by the vet. I know aluminum based ones are better binders, but hard to find any in UK. If anyone can recommend one that can be bought easily in UK, please feel free to suggest it.
Ottie always drink water, so never had to worry about him drinking water. I do keep an eye on how much he drinks though. Ottie is on wet food only, and when he was on renal food he did not drink water. He started drinking water once we went off the renal food to low carb food. Recently, when he has been eating Thrive, he seems to drink more. I don't know why though.
I just want Ottie to feel better... but I'm often confused which is causing him to be mopy. As far as I know... the symtoms of both diabetes and CKD are very similar.
Suzanne & Darcy
Member Since 2020
Epakitin is okay to use as a phos binder as long as his calcium levels are high. It can work for moderately elevated phosphorus, but for higher levels you need the aluminum hydroxide type binders.
Suzanne & Darcy
Member Since 2020
You may end up having to feed the renal food and just adjusting his insulin accordingly to keep his BG under control. Some people have to do this (I did.)
Kili
Member Since 2023
You may end up having to feed the renal food and just adjusting his insulin accordingly to keep his BG under control. Some people have to do this (I did.)
The problem with renal food was that Ottie initially loved it, and then after a week he just refused to eat it. Renal food is very high in carbs (20%+)... I think I initially had this question at the beginning...
Whether treating the diabetes takes precedence or CKD. It appeared that people believed that treating the diabetes takes priority because it's the more immediate threat, whilst CKD is harder to manage.
Could you give some indication of how you have managed to handle your kitty's CKD?
Elizabeth and Bertie
Member Since 2010
Some of us in the UK do have vets who will give us meds to use at home as we deem necessary. From what I've observed this seems to be becoming more common now, thank goodness.. My diabetic cat has CKD and pancreatitis. And my vet lets me have a supply of Cerenia and Mirtazapine.If you were in the US, I would say to get some Cerenia tablets and also some Ondansetron tablets from your vet (or a script to purchase them) but my friends in the UK often aren’t able to get these meds to take home and treat at home.
I get aluminium hydroxide from Hyperdrug.I know aluminum based ones are better binders, but hard to find any in UK. If anyone can recommend one that can be bought easily in UK, please feel free to suggest it.
Eliz
Kili
Member Since 2023
I get aluminium hydroxide from Hyperdrug.
Can you share the name of the product? Is it safe for cat usage?
Is it that much better than Ipakitine which is calcium based?
Some other member also suggested me Nefrokrill, Renvela, and Pronefra.
I don't know what type they are, but I know Pronefra is calcium based still.
Last edited:
Elizabeth and Bertie
Member Since 2010
https://hyperdrug.co.uk/aluminium-hydroxide-powder-30g/#feefo-product-review-widgetIdCan you share the name of the product? Is it safe for cat usage?
I base my dosage on the info from the 'Tanya' CKD site (my vet also recommends this site). See this page, and scroll down for recommended dosage for aluminium hydroxide.
http://felinecrf.org/phosphorus_binders.htm#dosage
Eliz
Kili
Member Since 2023
https://hyperdrug.co.uk/aluminium-hydroxide-powder-30g/#feefo-product-review-widgetId
I base my dosage on the info from the 'Tanya' CKD site (my vet also recommends this site). See this page, and scroll down for recommended dosage for aluminium hydroxide.
http://felinecrf.org/phosphorus_binders.htm#dosage
Has your kitty had some side-effects from taking the supplement?
Elizabeth and Bertie
Member Since 2010
Nope, no side effects.Has your kitty had some side-effects from taking the supplement?
Kili
Member Since 2023
Nope, no side effects.
At the moment, I'm struggling to feed Ipakitine twice a day. I presume this supplement is once daily?
I guess it's mixed with food like always. Did you start on 30mg per kg?
Suzanne & Darcy
Member Since 2020
My jar says:
Feed 1 scoop (1 gram) per 10 lbs. body weight twice daily with food.
I always added it to the morning and evening food.
Feed 1 scoop (1 gram) per 10 lbs. body weight twice daily with food.
I always added it to the morning and evening food.
Kili
Member Since 2023
This is very confusing.
Recently, I have increased dosage for Ottie back up to 0.25U. This morning, he seems fine and his BG doesn't seem to fluctuate that much.
HOWEVER... his second time his PMPS is 13.4, and after +2hrs it drops drastically to 3.8. Is this dosage still too high?
Luckily Ottie is eating. Do I feed him as much as he wants to eat? He just seems to eat non-stop. He probably feels a low drop in BG, but I'm trying to not stuff him so that his BG doesn't spike again like my prior hypo situations.
Recently, I have increased dosage for Ottie back up to 0.25U. This morning, he seems fine and his BG doesn't seem to fluctuate that much.
HOWEVER... his second time his PMPS is 13.4, and after +2hrs it drops drastically to 3.8. Is this dosage still too high?
Luckily Ottie is eating. Do I feed him as much as he wants to eat? He just seems to eat non-stop. He probably feels a low drop in BG, but I'm trying to not stuff him so that his BG doesn't spike again like my prior hypo situations.
.:. in.active .:.
Member Since 2023
I was going to suggest to find an in-between dose, but I can see you've already put in a provisional 0.2 IU for tomorrow.
His AM 0.25 numbers don't see much different than his AM 0.1 numbers, apart from his higher PMPS. Do you think, he may have bounced somewhere in the AM cycle (as in gone to lime green and intuitively eaten and/or the "panicky liver syndrome" kicked in and brought him higher for the pre-shot)?
But yes, dropping so quickly suggests that he may need a lower dose.
IF he were to drop below 3.8 tonight, I'd personally try for a 0.15 IU tomorrow instead of the 0.2 IU. (Unless of course the more experienced members are around to see this and reply before your AM shot is due, and suggest otherwise.)
These 0.05 increments may seem tiny to us, but I can see huge differences in my own boy's numbers.
Did you end up buying digital callipers as I mentioned in a DM before, so you'd be able to microdose these tiny amounts?
Did you feed him at PM +2 or did he intuitively go and eat around this time? And if so - did he eat before you tested him for that +2 or after? Because this is obviously important, given that number is on the borderline.
And have there been any other changes? As in, him eating a lower carb dinner compared to AM or re: other supplements taken/not taken etc that could possibly have an effect on the steep drop?
Re: eating non-stop - did you mean this PM or in general? If general: do you reckon it has to do with his CKD, like a flair up or something? Because looking at his numbers I doubt it's related to high BG, unless of course there are higher numbers we don't see, or as you say -if it's a today PM thing only- intuitive eating re: steep glucose drop.
His AM 0.25 numbers don't see much different than his AM 0.1 numbers, apart from his higher PMPS. Do you think, he may have bounced somewhere in the AM cycle (as in gone to lime green and intuitively eaten and/or the "panicky liver syndrome" kicked in and brought him higher for the pre-shot)?
But yes, dropping so quickly suggests that he may need a lower dose.
IF he were to drop below 3.8 tonight, I'd personally try for a 0.15 IU tomorrow instead of the 0.2 IU. (Unless of course the more experienced members are around to see this and reply before your AM shot is due, and suggest otherwise.)
These 0.05 increments may seem tiny to us, but I can see huge differences in my own boy's numbers.
Did you end up buying digital callipers as I mentioned in a DM before, so you'd be able to microdose these tiny amounts?
Did you feed him at PM +2 or did he intuitively go and eat around this time? And if so - did he eat before you tested him for that +2 or after? Because this is obviously important, given that number is on the borderline.
And have there been any other changes? As in, him eating a lower carb dinner compared to AM or re: other supplements taken/not taken etc that could possibly have an effect on the steep drop?
Re: eating non-stop - did you mean this PM or in general? If general: do you reckon it has to do with his CKD, like a flair up or something? Because looking at his numbers I doubt it's related to high BG, unless of course there are higher numbers we don't see, or as you say -if it's a today PM thing only- intuitive eating re: steep glucose drop.
Last edited:
Suzanne & Darcy
Member Since 2020
If you use U-100 syringes then you can draw different doses. Are you still using the U-40s?
.:. in.active .:.
Member Since 2023
Yeah I'm an idiot lol, Suzanne definitely has the easier solution for you 
Suzanne & Darcy
Member Since 2020
Huh? I don't know what you are talking about or if this is a joke. I'm just trying to find out which syringes she's currently using since there was discussion on previous days about switching to U-100s and then she said she couldn't get any at that time... which was several days ago.Yeah I'm an idiot lol, Suzanne definitely has the easier solution for you
I'm just pointing out (as we've talked about before) that it's easier to draw a .2 units of ProZinc with a U-100 syringe.
Anyway, Kili, I'll be over on the ProZinc forum.
Kili
Member Since 2023
I currently have no U100 syringes and have a lot of the U40 syringes.
I am trying my best to measure smaller dosage but it's not easy. All I can guarantee is that the dosage is smaller than 0.25U.
At the moment Ottie's nadir seems to sit at 8.4 - 8.6 which I thought was too high, so I tried to increase dosage, but that seems like a no go situation.
I am trying my best to measure smaller dosage but it's not easy. All I can guarantee is that the dosage is smaller than 0.25U.
At the moment Ottie's nadir seems to sit at 8.4 - 8.6 which I thought was too high, so I tried to increase dosage, but that seems like a no go situation.
.:. in.active .:.
Member Since 2023
Huh? I don't know what you are talking about or if this is a joke. I'm just trying to find out which syringes she's currently using since there was discussion on previous days about switching to U-100s and then she said she couldn't get any at that time... which was several days ago.
Yeah I suggested the U100s too, if you recall.
I referred to my reply, which is right above yours - where I asked her about the digital calliper for fine dosing. Which is obviously less convenient than using U100s. That is all.
I currently have no U100 syringes and have a lot of the U40 syringes.
I'd either get U100s and if you have a lot of U40s put those (or some) on eBay for sale.
Or, if you rather use the U40s, as mentioned above - Prime a pair of callipers. I can DM you the link for what I've got. Cheap and works exactly how it should.
Suzanne & Darcy
Member Since 2020
Yes. I do remember you suggesting U-100s too -- a while ago back when the subject first came up. And yes, some people do like the digital calipers a lot for fine dosing.Yeah I suggested the U100s too, if you recall.
I referred to my reply, which is right above yours - where I asked her about the digital calliper for fine dosing. Which is obviously less convenient than using U100s. That is all.
I'd either get U100s and if you have a lot of U40s put those (or some) on eBay for sale.
Or, if you rather use the U40s, as mentioned above - Prime a pair of callipers. I can DM you the link for what I've got. Cheap and works exactly how it should.
- Status
- Not open for further replies.