Sam sure is being a bit of a diva, isn't he? Skyrocket to the moon, then plunge back to earth, all in one cycle....LOL
Just a housekeeping note...On your spreadsheet for 12/15, the number you
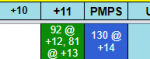
actually shoot is always the Pre-shot....so the 130 would be his PMPS. The way most of us enter it would be to enter 130 @ +14 in the PMPS cell....that way, the + cells still correspond to the number of hours since the SHOT.
You can either "stack" the other tests in the PMPS cell too (like 92 @ +12, 81 @ +13, 130 @ +14.....but you will have to color code it manually....in this case, the blue since that's the color that goes with the 130) OR you can put the 92 and 81 in the +11 cell like 92@+12, 81@+13 (and color code it the green) like this:
View attachment 65876